Most cases of colon cancer start as polyps. The opposite is not true: not all polyps turn into cancer. However, just to be sure it’s better to remove them and analyze them. Then, we have different options depending on how advanced the tumor is.
What is colon cancer?
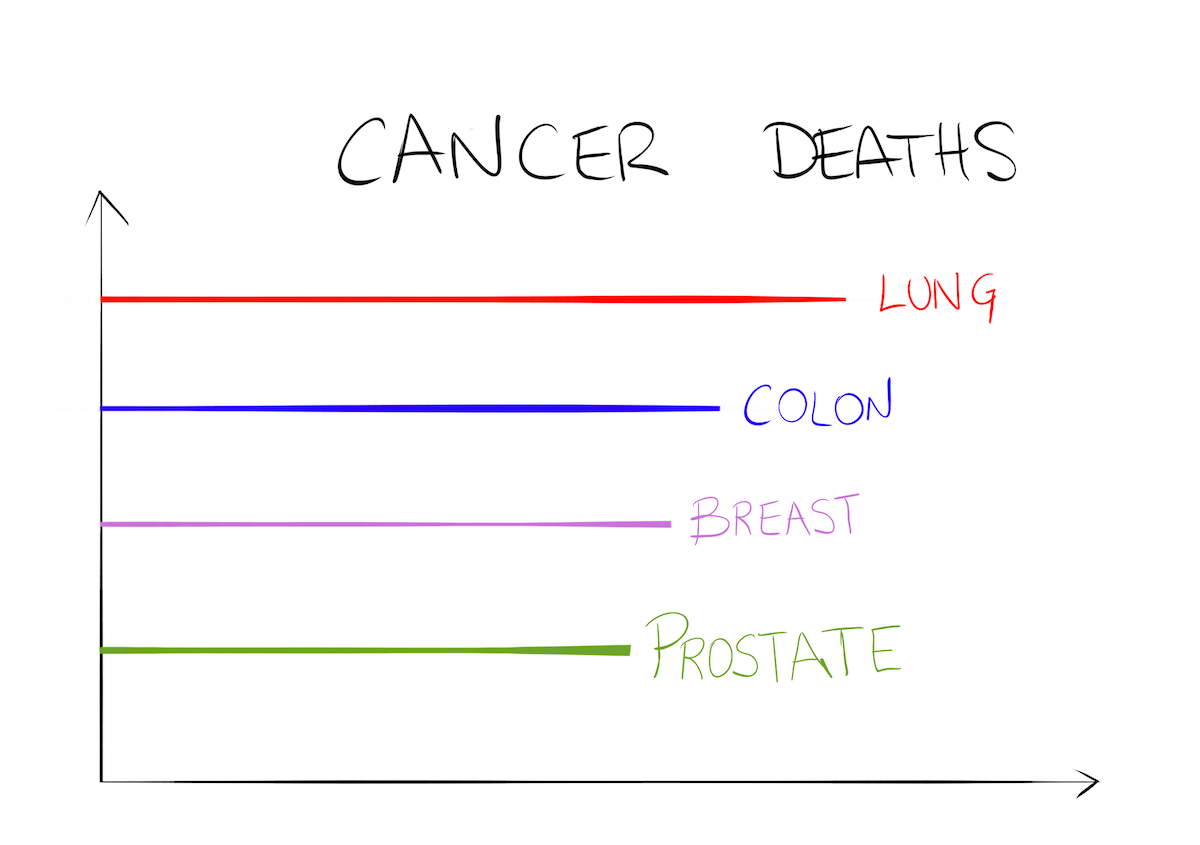
Colon cancer is one that arises from the large bowel (colon). It’s one of the most common, coming third in frequency after prostate and breast cancer. Also, it’s the second cause of death cancer after lung cancer.
The chances of a person getting colorectal cancer are around 1 in 25: out of 25 random people, one of them will get colorectal cancer during their lifetime. Colon cancer kills many people every year, over 50.000 people in EEUU. However, when we detect it early and treat it on time, the prognosis improves.
What are the symptoms of colon cancer?
In the beginning, it’s only a polyp in the colon wall and it doesn’t cause any symptoms. As the polyp keeps growing and invading other structures, it will start to cause symptoms. For example, if it narrows the bowel, it can cause constipation or even intestinal obstruction. It can also cause pain, especially if it infiltrates the nerves around it. One important sign is finding blood in your poo. However, it usually comes in very small drops that are mixed inside the stools, so you won’t see them. Actually, there is a screening test based on this.
Screening tests for colon cancer
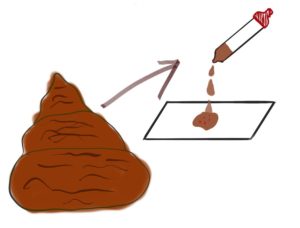
We use screening tests to find colon cancer before you have any symptoms. Unlike diagnostic tests, we don’t use them for one patient, but for whole populations. By screening so many people, we get to detect early cases of cancer. For colon cancer, we use the “fecal occult blood” test. The target population is adults from 50 to 75 years of age. First, you take a sample of your stool and place it in a special tube. Then you take the tube to the corresponding clinic or center, where they will look for occult blood. We are talking about microscopic drops, so you won’t see them by just looking. If they find some occult blood, you’ll need a colonoscopy. Sometimes, the colonoscopy will find a tumor or polyps, but not always. There can be other causes of occult blood like hemorrhoids, for example.
How do you diagnose colon cancer?
The best way is through a colonoscopy. A colonoscopy consists of a tube with a small camera attached. They insert it through your anus so that doctors can see your colon from the inside. If they find any polyps they’ll remove them, too. Then, they send them to the pathologist, who analyses to see if there are malignant cells in them.
Sometimes you may also need a CT. Unlike colonoscopy, CT can see the outside of the colon wall. It allows us to know if the tumor is infiltrating other organs around it. Besides, it can also find distant metastases.
What’s the staging for colon cancer?
It’s very important for us if the tumor has spread somewhere before choosing any treatment (this we call staging). Is the tumor a tiny polyp? Is it infiltrating other organs? Are there distant metastases?
As you can imagine, the treatment will be different for each case. A patient with just a polyp may be cured just by removing it through a colonoscopy. On the other side, the patient with metastases will need chemotherapy.
The main way to stage colon cancer is through a full body CT. It will show us if there is infiltration or metastases. The pathologists also play a role, because when they study the sample, they can check if there is microscopic infiltration of nerves, fat…
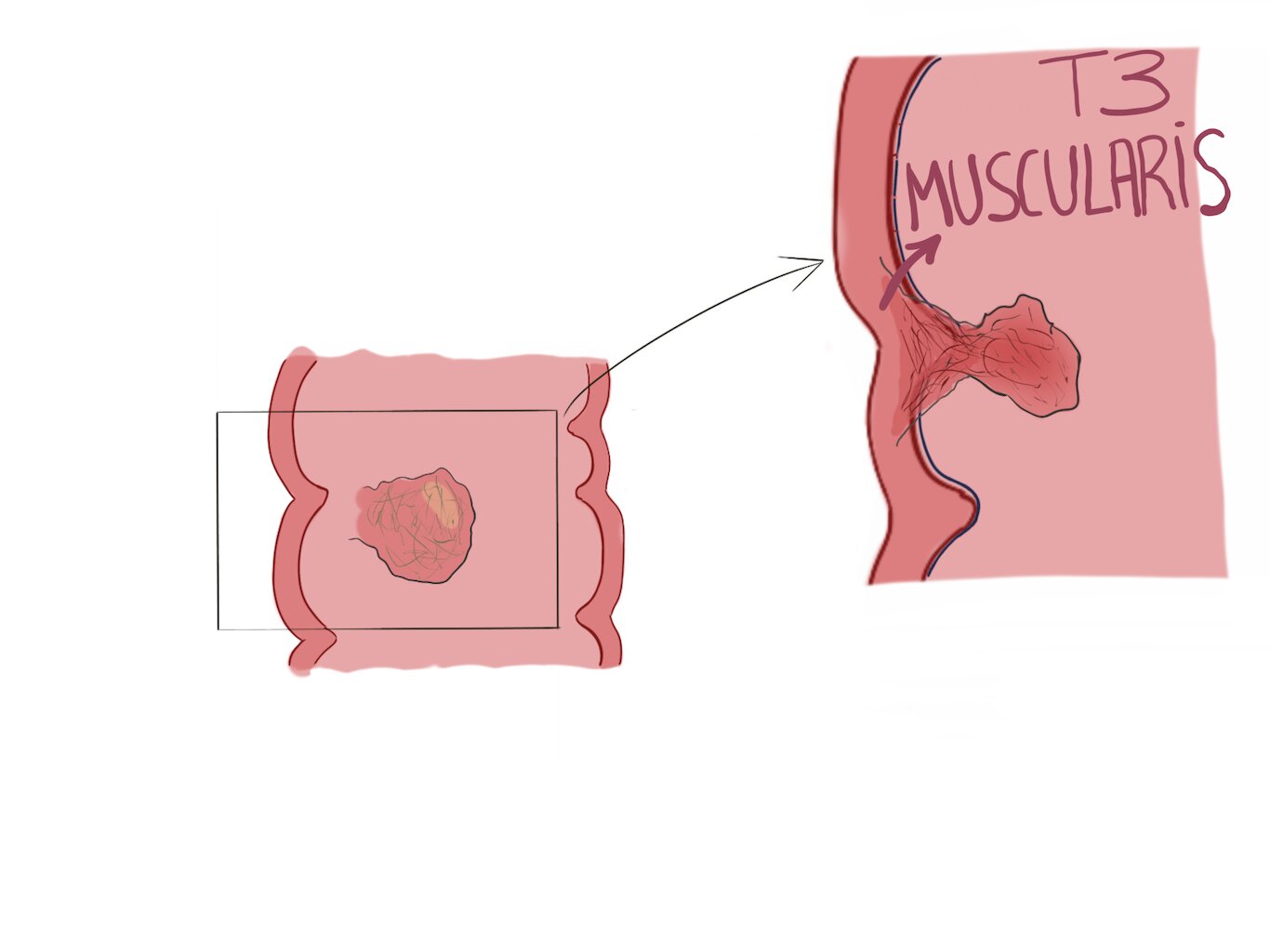
We need to know how deeply the tumor infiltrates. A “T1” tumor is superficial, “T4” tumor infiltrates the whole wall. Therefore, we need to be more aggressive with T4 infiltrating tumors.
How do you treat colon cancer?
It depends on the staging, so let’s see some different cases:
· A simple polyp
Colon cancer usually starts as a polyp. But not all polyps are malignant. In fact, most are benign. So how do we know which are malignant? We remove them and send them to the pathologist. If the pathologist finds tumoral cells but the borders of the polyp are clear, we’ve treated the tumor (it’s called endoscopic resection).
Sometimes the margins are affected but only in their most superficial layer (the mucosa). In these cases, surgeons can perform an endoscopic mucosal resection: they “peel” the affected mucosa through the endoscopy.
· Advanced tumors
For advanced tumors, we need more aggressive techniques, like surgery. Sometimes, we’ll use chemotherapy before surgery, to shrink the tumor (neoadjuvant chemotherapy).
Partial colectomy
They remove half of your colon (the one with the tumor). It can be a right or left hemicolectomy (depending on which side they remove).
Colostomy
Sometimes, doctors can’t reconnect both ends of the colon after surgery. In those cases, they may perform a colostomy: they attach one end to your abdominal wall. While you have it, you will poo through a small hole in your abdomen into a special plastic bag. These bags are watertight so that they are as clean and aseptic as possible.
Colostomy can be temporary or permanent. Sometimes, after a few months, they are able to finally reattach both ends of the colon, so they remove your colostomy. In other cases, reattachment is not possible and the colostomy is permanent.
Lymphadenectomy
If the tumor also affects your pelvic lymph nodes, they will remove them through surgery.
· Metastasic tumors
There are many different cases and they must be assessed individually. There are multidisciplinary committees in hospitals to discuss these cases. They are made up of oncologists, surgeons, gastroenterologists…
However, if there are metastases chances are you will need chemotherapy. Chemotherapy reaches all organs so it can kill malignant cells. We can also use chemotherapy to shrink a tumor before surgery (neoadjuvant). Sometimes we use it after surgery, to make sure there aren’t any malignant cells left (adjuvant).
New therapies
Targeted therapies
Chemotherapy is a great weapon against cancer, but it has side effects because it also attacks healthy cells in your body. It works through brute force.
Targeted therapies, as the name implies, only attack cancerous cells. If we find that the tumor has certain proteins on its surface, targeted therapies may be an option for that patient. We need a target therapy that’ll only attack those proteins. Unlike chemotherapy, targeted therapies are usually swallowed as a pill 💊.
Immunotherapy
Scientists discovered that, in order to develop cancer, malignant cells must first evade our immune system. In fact, our body kills many “baby tumors”.
To grow into cancer, those “baby tumors” must become invisible to our immune system, so that it won’t attack them. With immunotherapy, we try to wake up our immune system so that it can detect malignant cells again and start attacking them.
Prognosis
The prognosis for colon cancer depends greatly on the staging:
- The 5-year survival rate for localized colon cancer is 90%.
- For moderately invasive colon cancer, it’s 71%.
- Finally, if there are distant metastases, the survival rate is 15%.
Leave a Reply