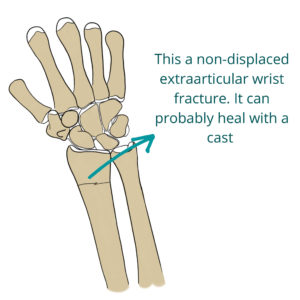
Wrist fractures are sometimes hard to tell from sprains, especially if they are non-displaced extraarticular fractures. Depending on the type of fracture, sometimes they need surgery and sometimes they don’t. Some of them heal fine with just a cast.
Table Of Contents
You can break your wrist when you fall on your outstretched hand. This can happen if you fall while practicing sports but also if you just slip and fall. Elder people are more prone to break their wrist, because their bones are weaker from osteoporosis.
There are several bones you can break in your wrist, but the most frequent one is the radius. In this post, we’ll be talking about distal radius wrist fractures. If you want to know about scaphoid fractures, you can read this post.
How do you know if it’s a fracture or just a sprain?
If your wrist is broken it’s usually very painful, you’ll have a deformity and won’t be able to move it. However, if it’s a small non-displaced fracture you may be able to still move it. You’ll just feel some pain, making it hard to differentiate from a sprain.
To really make sure whether or not you broke your wrist, you’ll need to go to the hospital for an x-ray. The x-ray will show the fracture most of the times.
However, if the fracture is too small and non-displaced, it can go unnoticed. For those cases, a C.T. or MRI will show fractures more accurately, even those “invisible” in the x-ray.
Types of wrist fractures
There are several types of wrist fractures, some of them even with their own name, like “Colles fracture”, the most common one. When classifying wrist fractures, surgeons look at several characteristics, like: are the fragments displaced? does it affect the joint surface? is it a stable fracture?
When to treat wrist fractures
In order to decide whether a fracture will need surgery, doctors have to consider both the patient condition and the fracture type.
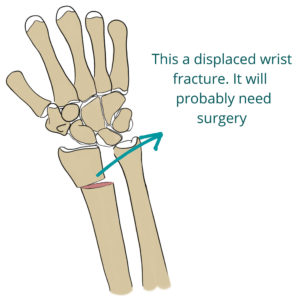
If the fracture has displaced fragments or is unstable, it will probably benefit from surgery. The opposite is true too: a non-displaced clean fracture with no joint involvement can be treated with a cast, as the fragments will stay together and heal.
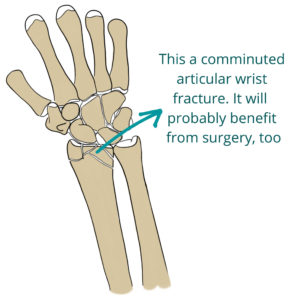
On the other side, a fracture that is displaced, comminuted, unstable or affects the joint, will benefit from surgical fixation.
Another important factor is the patient conditions. Surgery works best for young active patients. In the case of elderly people with little activity, a conservative treatment may be preferable, because surgery is risky for them (anesthesia, bleeding, infection…) and they don’t need a perfect range of motion (they are not going to play Roland Garros). It’s better to assume a small limitation in the range of motion than taking the risk of surgery.
Conservative treatment
With conservative treatment you will get a cast covering your wrist. We use it for non-displaced fractures and for patients not suitable for surgery (because the risks outweigh benefits).
Right before applying the cast, doctors will have to re-align the fragments if they were displaced. This is done under local anesthesia, and it is called reduction of the fracture.
Actually, even if you get surgery, they will first try to reduce the fracture in the emergency room. Try not to panic, because the procedure looks a little savage: one doctor ties some bandages around your fingers and wrist and starts pulling. Meanwhile another doctor is pulling from your elbow in the opposite direction. Sometimes a third one pushes your wrist to “place the fragments back together”. Despite anesthesia, it can be a little painful.
After that, your hand can swell. Try to keep your hand elevated above your head and move your fingers as if squeezing an invisible ball. This movement will activate your forearm muscles and help reduce swelling.
Surgery for wrist fractures
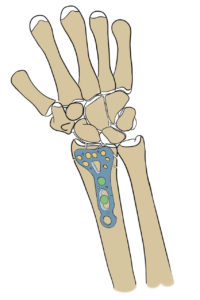
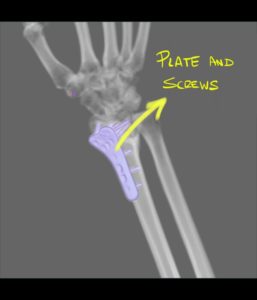
The most common surgical treatment is ORIF (Open Reduction Internal Fixation) with a plate. Open reduction means they have to open your forearm (surgery). Internal fixation means the plate will stay beneath the skin (as opposed to external fixation, which we’ll see next). The plate will be drilled into the different fragments, keeping them together and allowing the callus to form.

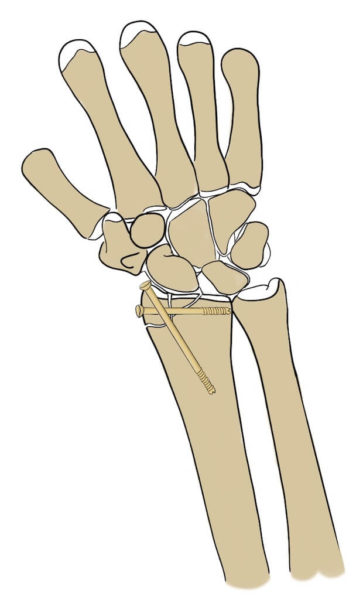
Screws for wrist fracture
Sometimes, depending on the characteristics of the fracture, screws may be more suitable than plates. For example, if the fracture is only affecting the tip of the radius (the styloid process). Anyway, your orthopedic surgeon is the one who will decide the best treatment.
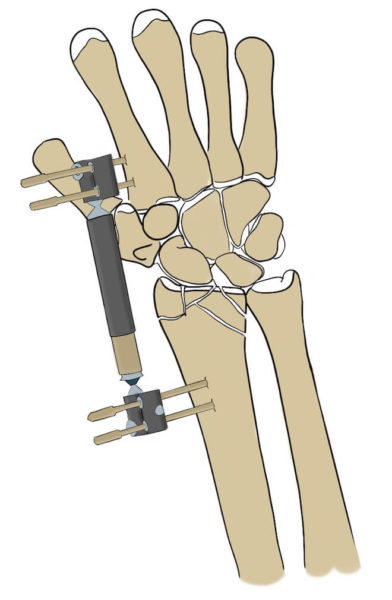
External fixation
External fixation is used for very comminuted fractures (really shattered ones) and for polytraumatized patients.
If the fracture is very comminuted, there won’t be any bone to drill the plate to. So, external fixation allows us to stabilize the wrist by fixing the proximal and distal bones. It’s usually a temporary measure, until surgery is possible or until the fracture heals.
In the case of polytraumatized patients we use external fixation to stabilize the fracture while we treat more urgent lesions: cranioencephalic trauma, pelvic fractures… Once the patient is out of danger, we can perform definite surgery with plates or screws.
How to rehab wrist fractures
No matter if you got surgery or a cast, you will spend some weeks without moving your wrist. It’s important that you don’t lose too much mobility and range of motion, both in your fingers and wrist.
First, while you still have your cast on, you have to do the exercise of opening and closing your fist several times a day. You can get a sponge ball and squeeze it, doing several series every time. That way, you’ll minimize the loss of strength and mobility in your fingers.
Once you get your cast off, you’ll have to add some wrist exercises. Our wrist has 3 sets of motion:
- Flexo-extension: moving the palm up and down.
- Radial and cubital deviation: moving your hand “towards the sides”.
- Supination and pronation: twisting your hand pointing your palm up and down.
You will need to do several sets of all these movements. Grab your hands together and repeat all 3 sets of movements. That way, the healthy hand will help too.

These exercises are painful at the beginning, but they are worthy. So take it easy, do them smoothly and don’t push it. You’ll be able to do them better and better with time. After a little time and practice, if you are consistent, you’ll gain all your strength and mobility back.
Leave a Reply