Gastric cancer can be pretty aggressive once it grows to more than just a polyp. That’s why we want to detect it before it grows outside the stomach. The problem is, by the time it causes symptoms, it’s usually too late.
[box type=”shadow”]
About Gastric Cancer
[/box]
There are over 25.000 new cases of gastric cancer in the USA each year, although its frequency has declined in the past 10 years. Gastric cancer accounts for about 1.5 % of all new cancers in the USA.
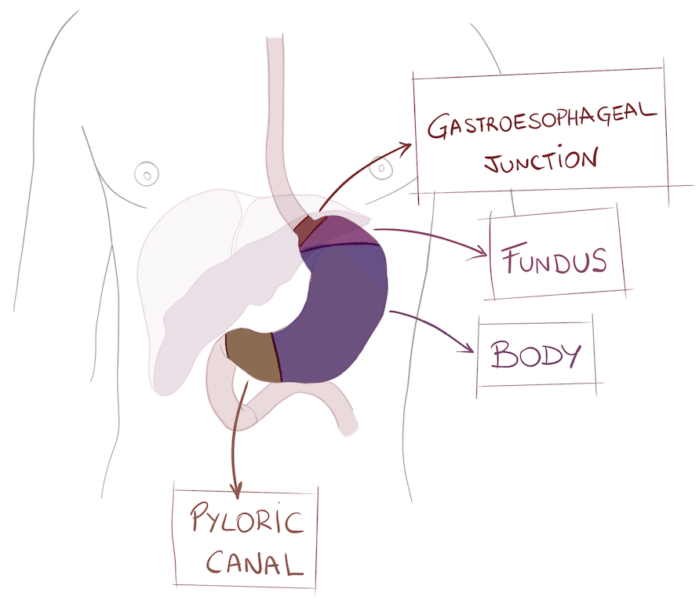
The stomach is part of the digestive tube, between the esophagus and the small bowel. It has a “bag” shape because it keeps food inside for hours and then releases gastric acids to digest it. It has several parts:
Gastric cancer usually starts as a polyp that grows until it becomes a mass or an ulcer. It is very aggressive locally, which means it grows and infiltrates the structures around it, making it hard to remove it completely.
What causes gastric cancer?
There are some main risk factors that increase the risk for for gastric cancer, like gastroesophageal reflux. Gastroesophageal reflux happens when food and gastric acid comes back up into the esophagus. If reflux happens for many years, it causes chronic injury, which can turn into cancer.
The way we eat can increase the risk, too. For example, obesity gives us a higher chance of gastric cancer. Also, some types of foods, like smoked salmon, increase the risk. We know this because there are some countries which eat a lot of smoked foods (like scandinavian countries) and they happen to have high rates of gastric cancer.
Family matters as well: if there are other cases of gastric cancer in your family, your risk increases.
There is a bacterium that lives in some peoples stomachs, Helicobacter pylori. It is VERY common. It lives in the stomach of millions of people, in some countries up to 80% of the population are infected. Most of the time it doesn’t cause any trouble, but in some cases, it causes gastritis, ulcers and, very rarely, cancer.
Finally, smoking. Smoking increases the risk for many diseases and tumors (like lung cancer, of course). Well, it’s also bad for gastric cancer.
What are the symptoms of gastric cancer?
If the tumor obstruct your stomach, you’ll get vomiting and nausea. Also, you can feel bloated after eating. It the tumor grows inside the stomach, it can give the illusion of feeling full of food. You can feel pain, which typically happens below the ribs and above the bellybutton. You can suffer weight loss, first because you can’t eat as much. Also, some tumors (including gastric cancer) cause constitutional syndrome, which is fatigue, anorexia and weight loss.
How do you diagnose gastric cancer?
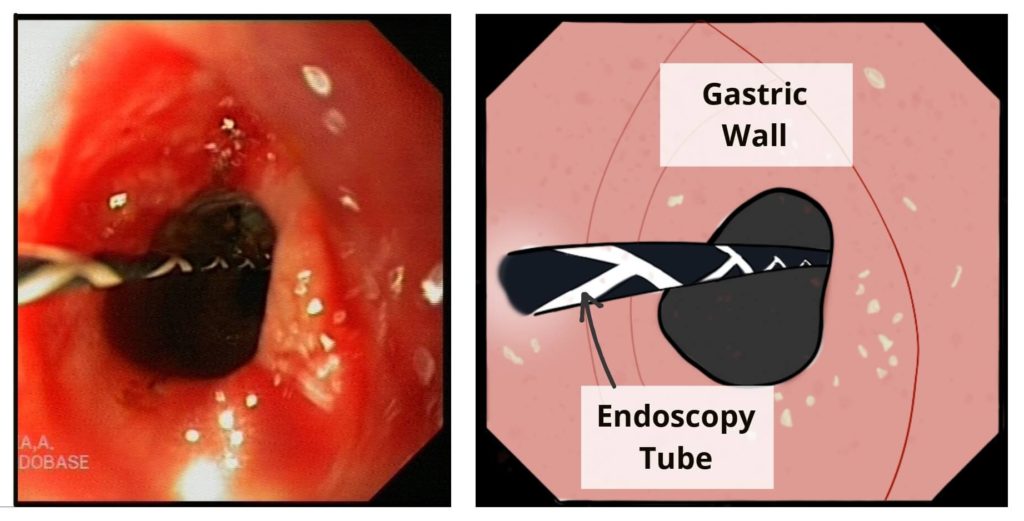
Endoscopy
The most accurate test is an endoscopy. Endoscopy consists of a flexible tube that is inserted through your mouth. It has a tiny camera attached to its end that shows everything on a screen. It allows your doctor to inspect your stomach from inside. Then, they can get a tissue sample through the same endoscope. That sample will be analyzed so that they can be sure it’s cancer.
Ecoendoscopy
Sometimes, if the tumor is growing outwards, we won’t see any tumor with the camera. In those cases we can use a ecoendoscopy, which is the same but with an ultrasound device on its tip. That way, doctors can see not only the gastric wall from inside, but they can also see what’s on the other side: they can see through the gastric wall.
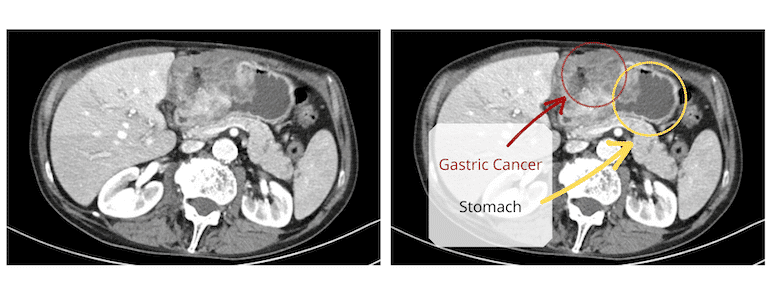
CT scanner
After making sure it is cancer, you’ll need a full body CT.
C.T. will depict the tumor and give information about it: is it infiltrating? Has it spread? Are there lymph nodes o metastases in other organs?
How do you treat gastric cancer?
As with most tumors, treatment depends on the staging. If the tumor has barely grown, removing the polyp may be enough. In most cases, however, it is necessary to remove part of, or the whole, stomach. After that, your oncologist may choose to add chemotherapy or radiotherapy.
Surgery
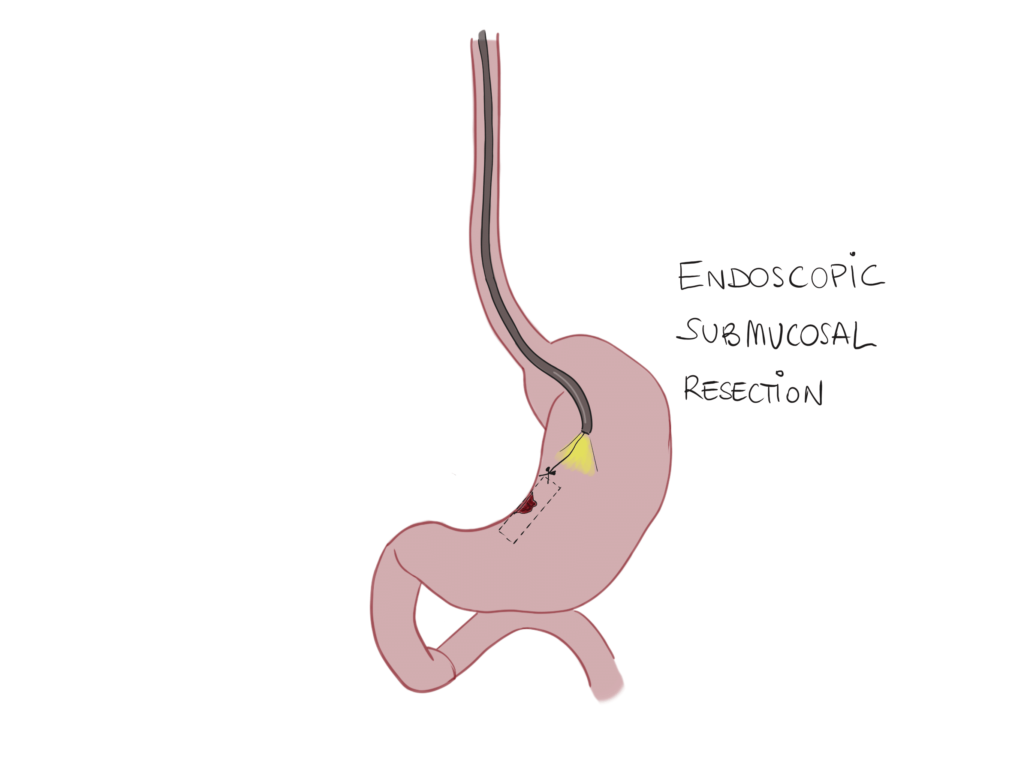
Endoscopic submucosal resection
If the tumor is only affecting the mucosa, then it can sometimes be removed through endoscopy. This procedure is called endoscopic submucosal resection. It consists of a peeling of the mucosa by cutting through the submucosal tissue. Unfortunately, most tumors are larger than that when they are diagnosed.
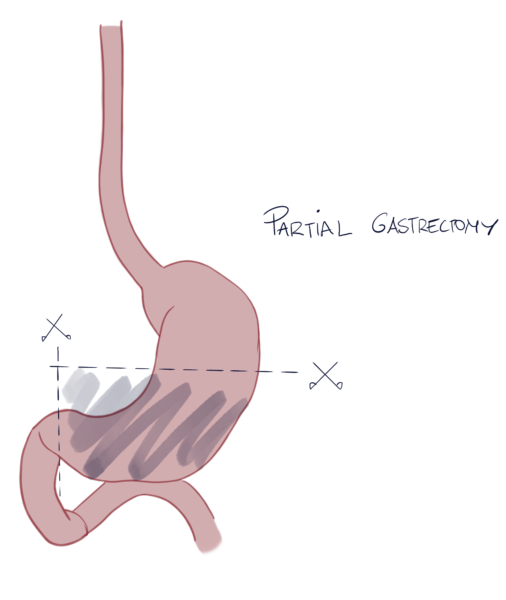
Partial gastrectomy
In most cases, they will remove at least part of your stomach. If the tumor is in the lower part of the stomach (pyloric canal) then surgeons might preserve the upper part of the stomach. That is called partial gastrectomy as they only remove one part of the stomach. Then they will reattach the upper part with the small bowel (the duodenum).
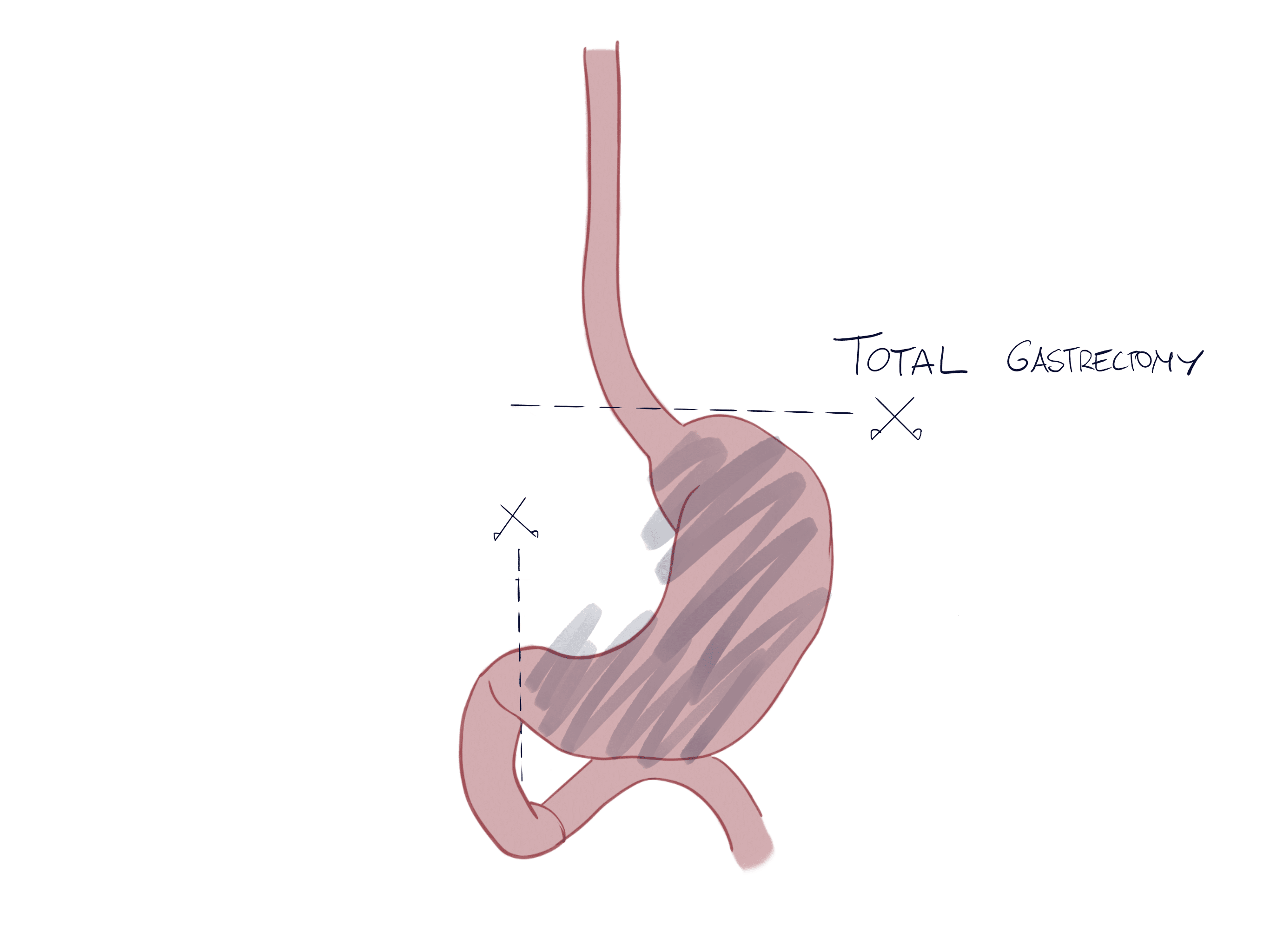
Total gastrectomy
If the tumor is located on the body or gastroesophageal junction, then they’ll have to remove your whole stomach: that is called total gastrectomy. Then, they will reattach your esophagus directly to your small bowel.
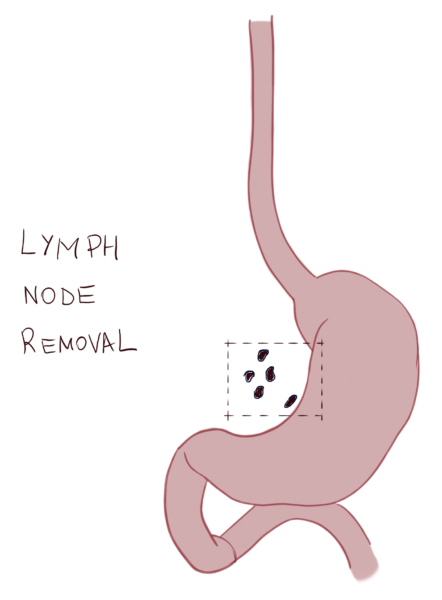
Lymph node resection
If the tumor has spread to local lymph nodes, your surgeon will also remove them during surgery. We call this lymph node resection or lymphadenectomy. It’s important because otherwise, malignant cells will keep spreading through the lymphatic system.
Chemotherapy
Chemotherapy works by traveling through your blood and killing any cell that is replicating fast. That includes tumoral cells, so it’s a great option to treat distant metastasis and advanced disease.
We can use chemotherapy in several ways. First, we can use it before surgery, to shrink the tumor. That is called neoadjuvancy. If it works, the tumor will be smaller and the surgeon will be able to remove it through surgery. It is used when the tumor is too large or too infiltrating. We also use it after surgery, to make sure it doesn’t come back. Because after removing the tumor, there may be microscopic malignant cells remaining. Chemotherapy will kill those cells and prevent recurrence (cancer coming back). Finally, another use for chemotherapy is when the tumor is too advanced and we can’t remove it. In those cases, chemotherapy will improve symptoms and survival (palliative).
Unfortunately, some of our own healthy cells also replicate fast and get damaged along the way (side effects). That is why patients lose their hair, have diarrhea…
Radiotherapy
Radiotherapy uses an external radiation beam to kill malignant cells. Like chemotherapy, it can also be used:
- To shrink the tumor before surgery.
- To kill any remaining cells after surgery.
- When the tumor is too large so we can’t remove it.
We use it combined with chemotherapy.
Targeted therapies
These are new promising therapies that are changing the way we treat cancer. Targeted therapies only attack certain cells, those that “carry” certain proteins. For each protein there is a different therapy. These are called targeted therapies. To use them, first, you have to make sure that the tumor is carrying some of the proteins. If it does, then you can give the patient the drug that will attack that specific protein. The main benefit of targeted therapies is that they only attack malignant cells. Conventional chemotherapy works as a war tank and targeted therapies as a sniper.
Nevertheless, we use them together (chemotherapy and targeted therapy), that way they are more effective.
Immunotherapy
They are drugs that reactivate our immune system, urging it to fight cancer again. See, tumoral cells know how to evade the “security system” our body uses to prevent cancer, which is part of the immune system. Tumor cells learn how to be invisible to our immune system. Otherwise, our white blood cells would kill them. With immunotherapy, we can make cancer visible again, so that our immune system starts attacking it again.
Leave a Reply